INTRODUCTION- The Zika virus belongs to the Flaviviridae family
and the Flavivirus genus, having a non-segmented
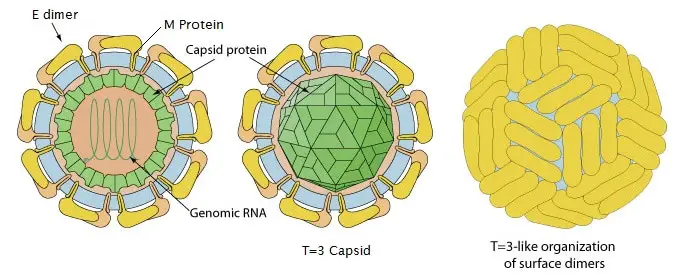
positive-sense Ribonucleic
acid (RNA) genome. The virus is about fifty nm in diameter,
enveloped and spherical, with an icosahedral like arrangement of surface
proteins. It is named as “Zika Forest” and is found close to capital of Uganda. Over the past few months, it has rapidly
emerged in the Western Hemisphere [1]. This virus is alike to different member
viruses of the family Flaviviridae, including yellow fever virus, dengue virus
and West Nile virus that causes symptoms like ill health in conjunction with rashes.
It conjointly shares
similar characteristics with the Spondweni virus [2].
.jpg)
Fig.
1: Structure of Zika virus
Source: http://laboratoryinfo.com/wp-content/uploads/2016/01/zika-virus.jpg
{kind=link}
ZIKV is transmitted to human beings through the bite
of daytime-active Aedes mosquitoes; however, infection threat through
sexual activity and blood transfusions also exists [3-5]. Phylogenetic
analyses of ZIKV virus suggested two significant lineages, Asian and African,
originating from a single ancestor, most likely in Uganda [3]. The
possible vectors of Aedes species include Aedes polynesiensis and
Aedes aegypti, identified in French Polynesia, and Aedes
hesilli, identified in Yap [4,6-7]. Aedes albopictus and A.
aegypti exist in many states of America, including various parts of the
south-central and south-eastern USA and Hawaii [1,4].
The RNA of the virion is infectious and acts as viral
messenger RNA (mRNA) and viral genome. The genome is translated as a
polyprotein through a length of 3419 amino acids as well as is processed co and
post-translationally by the both host and viral proteases [8]. The
ZIKV reproductive cycle begins with the attachment of the virion to the cell
membrane of the host via an envelope protein that encourages endocytosis. After
endocytosis, the viral membrane fuses with the endosomal membrane, and the
single-stranded RNA (ssRNA) is discharged into the cytoplasm of the host cell
then, translation begins and a polyprotein is cleaved, which is implicated in
the development of all structural along with nonstructural proteins.
Replication occurs during the further step, which occurs in the cytoplasmic
viral factories of the endoplasmic reticulum (ER), producing double-stranded
RNA (dsRNA). This dsRNA undergoes transcription to form additional ssRNAs,
which assemble within the ER to form new virions. These virions are then
transferred to the Golgi body apparatus and are ultimately discharged into the
intracellular spaces, where they cause infection of novel cells [9].
Table
1: Genome
structures of ZIKV strains
|
S. No. |
|
Length |
|
|
Gene
or genomic region |
African
MR 766 prototype straina [10] |
French
Polynesia H/PF/2013b [11] |
|
|
|
5= NCR |
106
ntc |
107
nt |
|
|
Capsid |
122
aad |
105
aa |
|
|
PrM |
178
aa |
187
aa |
|
|
Envelope |
500
aa |
505
aa |
|
|
NS1 |
342
aa |
352
aa |
|
|
NS2A |
226
aa |
217
aa |
|
|
NS2B |
130
aa |
139
aa |
|
|
NS3 |
617
aa |
619
aa |
|
|
NS4A |
127
aa |
127
aa |
|
|
NS4B |
252
aa |
255
aa |
|
|
NS5 |
902
aa |
904
aa |
|
|
3’ NCR |
428
nt |
428
nt |
|
|
Complete
genome |
10,794
nt |
10,617
nt |
aData collected from Kuno G & Chang [10]
bData collected from Baronti et al.
[11]
cnt, nucleotides
daa,
amino acids
Classification and Phylogeny of ZIKV- ZIKV is sited in to the clade X mosquito-borne Flavivirus
cluster, along with SPOV [12]. These outcome, based on
incomplete sequencing of the gene for nonstructural protein 5 (NS5), were
established by sequencing the complete coding region of the NS5-encoding gene [13].
The full genome of ZIKV (ZIKV MR 766 prototype strain) was completely sequenced
for the initially in 2007 [14]. The full sequences of other ZIKV
strains from Cambodia, Brazil the Central African Republic, Malaysia, Puerto
Rico, Senegal, Nigeria, French Polynesia, Thailand, Guatemala, and Yap State
are available in GenBank (http://www.ncbi.nlm.nih.gov/GenBank/) [13,15-17].
The genome structures of the ZIKV MR 766 prototype strain and the French
Polynesian H/PF/2013 strain are detailed in Table 2. ZIKV, similar to another
flaviviruses, is a single-stranded (ss), positive-sense RNA virus with a genome
of 10,794kb [14,18] with two flanking non-coding regions (5= NCR and 3= NCR). The open reading frame (ORF)
encodes a polyprotein with 3 structural proteins, i.e. capsid (C), pre-membrane (PrM), and envelope (E), and 7
nonstructural proteins, NS1, NS2A, NS2B, NS3, NS4A, NS4B, & NS5 [14].
Phylogenetic
analysis was shown that Zika virus can be divided into distinct African and
Asian lineages; equally emerged from East Africa during the late 1800s or early
1900s [19].
The Asian lineage originated during the virus’s migration from Africa to
Southeast Asia, where it was initial detected in Malaysia. From there, Zika
virus spread to the Pacific Islands, separately to
Yap and French Polynesia, and then to New Caledonia, Cook Islands, Easter
Island, and the Americas [19].
.jpg)
Fig. 2: Phylogenetic tree of ZIKV showing the
African and Asian lineages, including the strains that recently emerged in the
Pacific and Brazil [20]
Virology and Pathogenesis- Zika virus is a positive-sense single-stranded RNA (ssRNA) virus
belonging in the family of Flaviviridae, which includes numerous other
mosquito borne viruses of medical importance (e.g. WNV, DENV, & yellow
fever virus [YFV]) [21]. Its
neighboring relative is Spondweni virus, another member of its clade [21-22]. The Zika virus genome
contains 10,794 nt encoding 3,419 aa [22]. Like other flaviviruses, Zika virus is composed of 2
non-coding regions (5′ and 3′) that flank an open reading frame [22], which encodes a
polyprotein cleaved into the capsid, precursor of membrane, envelope, and 7
nonstructural proteins [22].
Zika virus’s molecular
evolution studies is based on viral strains collected from four different
countries in West Africa duration of 1947-2007, identified numerous sites
within Zika viral genome, were under well strong negative selection pressure.
This result suggested that frequent purging of deleterious polymorphisms in
functionally essential genes and the possibility of recombination, which
present rarely amongst flaviviruses [23]. The implications of this result require further
estimation with respect to viral spread, zoonotic maintenance, and
epidemiologic potential.
After mosquito inoculation
of a human host, cellular entry likely resembles that of other flaviviruses,
whereby the virus enters skin cells through cellular receptors, enabling
migration to the lymph nodes and bloodstream. Few studies have investigated the
pathogenesis of Zika virus infection. One study showed that human skin
fibroblasts, keratinocytes, and immature dendritic cells allow entry of Zika
virus [24]. Several
entry and adhesion factors (e.g. AXL receptor tyrosine kinase) facilitate
infection, and cellular autophagy, needed for flaviviral replication, enhances
Zika virus replication in skin fibroblasts [24]. After cellular entry, flaviviruses typically
replicate within endoplasmic reticulum-derived vesicles. However, Zika virus
antigens were found exclusively in the nuclei of infected cells; this finding suggests
a location for replication that differs from that of other flaviviruses and
merits further investigation [25].
Vectors and Transmission- A vector of arboviruses
may be definite as an arthropod that transfers the virus from one vertebrate to
other vertebrate by bite [26].
The most ordinary approach of biological transmission is infection during a
viremic blood meal and injection of infectious saliva during blood feeding
(horizontal transmission). Non-vector arbovirus transmission has been reported to
occur straight between vertebrates [27-28],
from mother to child [29-34], nosocomially [35–37], by
transfusion [38–41], via bone marrow [42] or organ transplantation, and sexually.
Health Care Worker Prevention- Health care workers practicing may face distinctive health
hazards. Varied infectious
risks area unit related to patient
contact or handling clinical specimens. varied sorts of health
care workers is also at
risk: Physicians, nurses, and alternative adjunct clinical employees providing care in international
settings, as well as clinics,
hospitals, and field locations, Medical students and alternative health care
trainees participating in
clinical rotations overseas, Other
people working in clinics, hospitals, or laboratories, as well as researchers,
laboratory technicians, adjunct
employees, and public health workers. Risks vary deepending on the duties of
the employee, the
geographic location, and therefore
the practice setting.
Increase risks area unit attributable to multiple factors as well as the following:
·
Less stringent safety rules or infection management standards.
·
Limited availability of
personal protective equipment (PPE) or safety-engineered devices.
·
Unfamiliar practice conditions or instrumentation.
·
Challenging practice
conditions that can prevent providers from adhering to standard precautions
(such as extremely resource-limited settings, natural disasters, or conflict
zones).
·
Unfamiliar medical procedures.
·
High prevalence of
transmissible (such as HIV, hepatitis B, hepatitis C, or TB).
·
Potentially high infectious
burden and increased transmission risk from source patients (such as high HIV
viral loads in untreated patients).
·
Limited resources for
evaluation and treatment after exposure to bloodborne pathogens.
·
Potential to encounter uncommon
or emerging infectious diseases that are highly transmissible in health care
settings (such as Middle East respiratory syndrome [MERS] or Ebola virus
disease).
·
Increased psychological
stress resulting from practicing in resource-limited settings, isolated areas,
and long-term assignments.
These challenges should be taken into account by all health care
workers when they consider and prepare for international missions [43].
Management commitment
and employee involvement - Essential to implement
effective infection management programs selected personnel should review, update and act on all steerage, as well as normal operational procedures and
exposure management plans,
and should communicate
those policies and practices to
any or all employees. Early identification procedures/signage will facilitate to quickly establish suspect cases.
Healthcare workers
must receive training and education on
Zika identification and control. In addition to awareness training, personnel
who are at risk should receive training on how properly don and doff their
personal protective equipment [44].
.jpg)
Fig. 3: Zika Virus
Transmission Cycle
Clinical Manifestation-
Many
people infected with Zika won’t have symptoms or will only have mild symptoms.
The most common symptoms are fever, rash, headache, joint pain, red eyes, and
muscle pain. Symptoms can last for several days to a week. Once a person has
been infected with Zika, they are likely to be protected from future
infections.
Differential Diagnosis- In
the lack of other arbovirus epidemics, diagnosis can be solely made on clinical
grounds; however, as mentioned earlier, ZIKV outbreaks are generally linked
with other arbovirus epidemics making diagnostic investigations an essential
for clarifying the medical presentation [45].
Serological analysis- Detecting
IgM in the serum of patients by ELISA procedure is a valuable process, but
unavailable in many laboratories. Moreover, the cross reactivity with
antibodies to another arboviruses decreases the specificity of this technique [46-48].
In a recent study, serum samples from twenty-one patients with acute
undifferentiated fever in Thailand were examined for immune reactivity against
the Zika virus, Japanese encephalitis, Dengue, and Chikungunya envelope
antigens. This inversion was showed evidence of immunoreactivity against ZIKV
envelope, suggesting that the Zika virus outbreak might have transmitted to
Thailand [49].
However, due to the cross reactivity of serological analysis, more specific
investigative process (e.g. molecular diagnosis using real time PCR) are
necessary.
Molecular diagnosis (RT-PCR)- Molecular
diagnosis could be performed by the using of Reverse Transcriptase Polymerase
Chain Reaction (RT-PCR) [50].
These diagnostic studies were recommended that serum can give positive test for
viral particles and the illness as soon as fever appear, other than when the
rash occurs, viremia starts to drop. However, viral nucleic acids remain
detectable for about 20- 60
days from the onset of symptoms [51-52].
During the French Polynesia epidemic, Kutsuna et al. [53] reported positive viral RNA in urine, while serum samples from the same
patients were negative. Gourinat et al. [48] were reported that
the virus could be detected in the infected individual’s urine samples of with
higher titers after 20 days from the onset of the illness. These result data
are consistent with former studies, which recommended prolonged finding of
viral RNA of another flaviviruses as dengue virus [54] and West Nile virus [55] in urine samples.
These reports emphasize the function of viral detection in urine as a
diagnostic technique for Zika viral infection during epidemics.
Treatment strategy- There is no specific treatment or antiviral drug for Zika
viral infection [56]. The present management guidance is based on a
limited body of facts. Recommendations are the handling of symptoms based on
acetaminophen for pain and fever, an antihistaminic for pruritic rash, and
drinking of fluids. Treatment with acetylsalicylic acid and nonsteroidal
anti-inflammatory drugs is discouraged because of the reported increased risk
of hemorrhagic syndrome with other flaviviruses (Secretariat of the Pacific Community,
http://www.spc.int/phs/english/publications/informaction/IA27/Zika-outbreak-Yap-2.pdf). In the initial days after onset of symptoms (viremic
phase), patient isolation to pass up mosquito bites is recommended to avoid the
infection to another people [56].
Prevention- No vaccine exists to
prevent ZIKV
in these days.
Avoid ZIKV by avoiding mosquito bites only. Mosquitoes that spread
ZIKV
by people
bite during the day
& night. Mosquitoes that spread ZIKV is also spread dengue and
chikungunya viruses. Zika can be passed through sex from a person, who
has Zika to his or her sex buddies. Condoms either male or female are able to
decrease the chance of getting Zika during sex. Local mosquito-borne Zika virus
transmission has been reported in the
continental US. The mosquitoes could spread Zika are found throughout the
US.
The
major vectors concerned in the spread and transmission of dengue, chikungunya,
and ZIKV are a broad range of Aedes mosquitoes. Therefore, preventive
measures begin with strategies intended to keep away from mosquito contact.
These strategies include drainage of mosquito breeding sites and use of
insecticides and N,N-diethyltoluamide (DEET) or picaridin
containing insect repellents. In addition the testing
of nucleic acid of blood donors, avoidance of
post-transfusion ZIKV can be performed by
microbial pathogen inactivation in blood products [57]. To moment, none vaccines have been made up
till now. But it is expected that the ZIKV 3 vaccine would encounter the same
problems of arbovirus vaccines owing to the 4 sporadic & unexpected
eruptions of epidemics; therefore, vaccinating a large five populations for
fear of its outbreak might not be cost-effective [58].
CONCLUSION-
Zika
virus is a flaviviruses which is transmitted
by the bites of mosquito (Aedes aegypti and some other species),
especially, during the day time. Zika virus can be
transmitted by sexual activity,
blood transfusions and from mother to child. Africa was considered the most
affected country followed by south and North America which reported ZIKV
cases recently. Zika infection is a pandemic that is spreading throughout
different parts of the world. Research preparedness is required on an immediate
basis to improve mosquito control procedures and to develop point-of-care
laboratory diagnostics, vaccines and antivirals that are appropriate to be used
in pregnant women. The main reason for ZIKV to become a global emergency is its
link with congenital birth defects (i.e. microcephaly) to infected mother and
lack of drugs or vaccines available due to very limited research and also an
absence of population immunity. The severe disease
associated with ZIKV in French Polynesia and Brazil, however, suggests that
this virus will become a very serious global public health problem due to lack
of any best vaccine against ZIKV infection. Continued vigilance is warranted, along with a concerted effort
toward improving our understanding, management, and prevention of this emerging
pathogen.
FUTURE
PROSPECT- Because of current explosive rise in Zika virus,
there is a dire need to carry out research based study to comprehend this
life-threatening disease and develop medical countermeasures. ZIKV illness is a
risk, not only to public health, but also to global security and economy. We
need to get serious about tracking Zika in patients who have traveled in south and Central
America and have symptoms. Prevention measures specifically vector
control are a current priority. Affordable insurance policy to develop experimental treatments
especially vaccines, against potential threats. However, there are
virus-specific therapeutic targets, which may lead to the improvement of
targeted anti-ZIKV drugs. In terms of treatment, the development of a broad
spectrum antiviral drug has been recently recommended because the "One
Bug-One Drug" approach is no longer practical. Because of the potential
for birth defects, pregnant women to stay out of places where the virus
is currently circulating. The association between Zika virus and
neurological manifestation require further verification. In addition, the
underlying pathological process and identification of population whom are at
risk of these neurological manifestations should be investigated in the future.
REFERENCES
1.
Chen LH, Hamer DH. Zika
virus: rapid spread in the Western hemisphere. Ann Intern Med. 2016; 164:613–5.
2.
Faye O, Freire CC, Iamarino
A, Faye O, de Oliveira JV, Diallo M, et al. Molecular evolution of Zika virus during
its emergence in the 20th century. PLoS Negl Trop Dis. 2014;
8:e2636.
3.
Lanciotti RS, Kosoy OL,
Laven JJ, Velez JO, Lambert AJ, Johnson AJ, et al. Genetic and serologic
properties of Zika virus associated with an epidemic, Yap State, Micronesia,
2007. Emerg Infect Dis. 2008; 14:1232–9.
4.
Hennessey M. Zika virus
spreads to new areas-region of the Americas, May 2015-January 2016. MMWR Morb.
Mortal. Wkly. Rep. 2016; 65:1031-4.
5.
Foy BD, Kobylinski KC,
Chilson Foy JL, Blitvich BJ, Travassos da Rosa A, Haddow AD, et al. Probable
non-vector-borne transmission of Zika virus, Colorado, USA. Emerg Infect Dis.
2011; 17:880–2.
6.
Cao-Lormeau VM, Roche C,
Teissier A, Robin E, Berry AL, Mallet HP, et al. Zika virus, French polynesia,
South pacific, 2013. Emerg Infect Dis. 2014; 20:1085–6.
7.
Duffy MR, Chen TH, Hancock
WT, Powers AM, Kool JL, Lanciotti RS, et al. Zika virus outbreak on Yap Island,
Federated States of Micronesia. N Engl J Med. 2009; 360:2536–43.
8.
Haddow AD, Schuh AJ, Yasuda
CY, Kasper MR, Heang V, Huy R et al. Genetic
characterization of Zika virus strains: geographic expansion of the Asian
lineage. PLoS Negl Trop Dis. 2012; 6:e1477.
9.
MicrobeWiki. Reproductive
Cycle of a Zika virus in a Host Cell. 2016. https://microbewiki.kenyon.edu/index.php/Zika_virus#cite_ref-g_5-1. Accessed 1 Mar 2016.
10. Kuno G, Chang GJ. Full-length sequencing and genomic characterization of Bagaza,
Kedougou, and Zika viruses. Arch Virol, 2007; 152:687–696.
11. Baronti C, Piorkowski G, Charrel RN,
Boubis L, Leparc-Goffart I, de Lamballerie X. Complete
coding sequence of Zika virus from a French
Polynesia outbreak in 2013. Genome Announc, 2014; 2:e00500-14.
12. Kuno G, Chang GJ, Tsuchiya KR, Karabatsos N, Cropp
CB. Phylogeny
of the genus Flavivirus. J Virol, 1998; 72:73–83.
13. Lanciotti RS, Kosoy OL, Laven JJ, Velez
JO, Lambert AJ, Johnson AJ, Stanfield SM, Duffy MR. Genetic and serologic properties of Zika virus associated with an epidemic, Yap State, Micronesia, 2007.
Emerg Infect Dis, 2008; 14:1232–1239.
14. Kuno G, Chang GJ. Full-length
sequencing and genomic characterization of Bagaza, Kedougou, and Zika viruses.
Arch Virol, 2007; 152:687–696.
15. Berthet N, Nakouné E, Kamgang B, Selekon B,
Descorps-Declère S, Gessain A, Manuguerra JC, Kazanji M. Molecular
characterization of three Zika
flaviviruses obtained from sylvatic mosquitoes in the Central African Republic. Vector Borne Zoonotic Dis, 2014; 14:862–865.
16. Vandenbogaert M, Cao-Lormeau V-M, Diancourt L,
Thiberge J-M, Sall A, Kwasiborski A, Musso D, Desprès P, Manuguerra J-C, Caro
V. 2014.
Full-length genome sequencing and analysis of 3 ZIKV strains on an Ion Torrent PGM sequencer, abstr
22.133. 63rd Am Soc Trop Med
Hyg (ASTMH) Meet, New Orleans, LA, 2 to 6 November 2014.
17. Lanciotti RS, Lambert AJ, Holodniy M,
Saavedra S, del Carmen Castillo Signor L. 29 January
2016. Phylogeny of Zika virus in Western
Hemisphere, 2015. Emerg Infect Dis http://dx.doi.org/10.3201/eid2205.160065.
18. Chambers T. 2008. Flaviviruses:
general features, p 241–252. In Encyclopedia of virology, 3rd ed.
Acadamic Press, New York, NY.
19. Gatherer D, Kohl A. Zika virus: a previously slow pandemic spreads
rapidly through the Americas. J Gen Virol. 2016; 97:269–73.
20.
Musso D, Gubler DJ. Zika Virus.
Clinical Microbiology Reviews, 2016; 29(3):487-524.
21. Lanciotti RS, Kosoy OL, Laven JJ, Velez JO, Lambert AJ,
Johnson AJ, et al. Genetic and serologic properties of Zika virus associated
with an epidemic, Yap State, Micronesia, 2007. Emerg Infect Dis. 2008;
14:1232–9.
22. Kuno G, Chang GJ. Full-length sequencing and genomic
characterization of Bagaza, Kedougou, and Zika viruses. Arch Virol. 2007;
152:687–96.
23. Faye O, Freire CC, Iamarino A, Faye O, de Oliveira JV,
Diallo M, et al. Molecular evolution of Zika virus during its emergence in the
20(th) century. PLoS Negl Trop Dis. 2014; 8:e2636.
24. Hamel R, Dejarnac O, Wichit S, Ekchariyawat P, Neyret A,
Luplertlop N, et al. Biology of Zika virus infection in human skin cells. J
Virol. 2015; 89:8880–96.
25. Buckley A, Gould EA. Detection of virus-specific antigen in the
nuclei or nucleoli of cells infected with Zika or Langat virus. J Gen Virol.
1988;69:1913–20.
26. World Health Organization. Arthropod-borne viruses. World Health Organ Tech Rep Ser, 1961;219:1–68.
27. Kuno G.
Transmission of arboviruses without involvement of arthropod vectors. Acta
Virol, 2001; 45:139-150.
28. Kuno G, Chang GJ. Biological transmission of arboviruses: reexamination of and new
insights into components, mechanisms, and unique traits as well as their
evolutionary trends. Clin Microbiol Rev, 2005;18:608–637.
29. Basurko C, Carles G, Youssef M, Guindi
WE. Maternal and foetal consequences of dengue fever during pregnancy.
Eur J Obstet Gynecol Reprod Biol, 2009; 147:29–32.
30. Tan PC, Rajasingam G, Devi S, Omar SZ. Dengue infection in pregnancy: prevalence, vertical transmission,
and pregnancy outcome. Obstet Gynecol, 2008; 111:1111–1117.
31. Fritel X, Rollot O, Gerardin P, Gauzere
BA, Bideault J, Lagarde L, Dhuime B, Orvain E, Cuillier F, Ramful D, Samperiz
S, Jaffar-Bandjee MC, Michault A, Cotte L, Kaminski M, Fourmaintraux A,
Chikungunya- Mere-Enfant Team. Chikungunya virus
infection during pregnancy,
Reunion, France, 2006. Emerg Infect Dis, 2010;16:418-425.
32. Gerardin P, Barau G, Michault A, Bintner
M, Randrianaivo H, Choker G, Lenglet Y, Touret Y, Bouveret A, Grivard P, Le
Roux K, Blanc S, Schuffenecker I, Couderc T, Arenzana-Seisdedos F, Lecuit M,
Robillard PY. 2008. Multidisciplinary prospective
study of mother-to-child chikungunya
virus infections on the Island of La Reunion. PLoS Med 5:e60.
33. Stewart RD, Bryant SN, Sheffield JS. West Nile virus infection in pregnancy. Case Rep Infect Dis, 2013; pp:1-3.
34. Centers for Disease Control and
Prevention (CDC). Possible West Nile virus
transmission to an infant through breast-feeding-Michigan, 2002. MMWR Morb
Mortal Wkly Rep, 2002; 51:877–878.
35. Wagner D, de With K, Huzly D, Hufert F,
Weidmann M, Breisinger S, Eppinger S, Kern WV, Bauer TM. 2004. Nosocomial acquisition of dengue. Emerg Infect Dis, 10:1872-1873.
36. Clark BM, Molton JS, Habib T, Williams
DT, Weston EL, Smith DW. Dengue virus infection in
Australia following occupational exposure: a reflection of increasing numbers of imported cases. J Clin
Virol, 2012; 54:376-377.
37. Nemes Z, Kiss G, Madarassi EP, Peterfi
Z, Ferenczi E, Bakonyi T,Ternak G. Nosocomial
transmission of dengue. Emerg Infect Dis, 2004; 10:1880–1881.
38. Tomashek KM, Margolis HS. 2011. Dengue: a potential transfusiontransmitted disease.
Transfusion 51:1654–1660.
39. Tambyah PA, Koay ESC, Poon ML, Lin RV,
Ong BK, Transfusion-Transmitted Dengue Infection Study Group. 2008. Dengue hemorrhagicfever transmitted by blood transfusion. N
Engl J Med, 359:1526-1527.
40. Stramer SL, Fang CT, Foster GA, Wagner
AG, Brodsky JP, Dodd RY. 2005. West Nile virus among
blood donors in the United States, 2003
and 2004. N Engl J Med, 353:451-
459.
41. Hoad VC, Speers DJ, Keller AJ, Dowse GK,
Seed CR, Lindsay MD, Faddy HM, Pink J. 2015. First
reported case of transfusion-transmitted
Ross River virus infection. Med J Aust, 202:267–269.
42. Rigau-Pérez JG, Vorndam AV, Clark GG. 2001. The dengue and dengue hemorrhagic fever epidemic in Puerto
Rico, 1994–1995. Am J Trop Med Hyg 64:67-74.
43. U.S.
Centers for Disease Control. Zika Virus. 1. USA. Gov/1Zv7N61.
44. Henry M. Wu, V. Ramana Dhara, Alan G. Czarkowski, Eric J. Nilles. Advising Travelers with Specific Needs. Chapter 8: Available from: https://wwwnc.cdc.gov/travel/yellowbook/2018/advising-travelers-with-specific-needs/health-care-workers; last updated: May 31, 2017.
45. Fauci
AS, Morens DM. Zika Virus in the Americas - Yet Another Arbovirus Threat. N
Engl J Med. 2016/01/14 ed. 2016.
46. Lanciotti
RS, Kosoy OL, Laven JJ, Velez JO, Lambert AJ, Johnson AJ, et al. Genetic and
serologic properties of Zika virus associated with an epidemic, Yap State,
Micronesia, 2007. Emerg Infect Dis. 2008;14(8):1232–9.
47. Dick
GWA, Kitchen SF, Haddow AJ. Zika virus (I). Isolations and serological
specificity. Transactions of the Royal Society of Tropical Medicine and
Hygiene. Oxford University Press; 1952; 46(5):509–20.
48. Gourinat
A-CC, O’Connor O, Calvez E, Goarant C, Dupont-Rouzeyrol M, O’Connor O, et al.
Detection of Zika virus in urine. Emerg Infect Dis. 2015; 21(1):84–6.
49. Wikan
N, Suputtamongkol Y, Yoksan S, Smith DR, Auewarakul P. Immunological evidence
of Zika virus transmission in Thailand. Asian Pacific journal of tropical
medicine. 2016; 9(2):141–4.
50. Faye
O, Faye O, Dupressoir A, Weidmann M, Ndiaye M, Alpha Sall A. One-step RT-PCR
for detection of Zika virus. J Clin Virol. 2008; 43(1):96–101.
51. Barzon
L, Pacenti M, Berto A, Sinigaglia A, Franchin E, Lavezzo E, et al. Isolation of
infectious Zika virus from saliva and prolonged viral RNA shedding in a
traveller returning from the Dominican Republic to Italy, January 2016. Euro
Surveill. 2016; 21(10):30159.
52. Corman
VM, Rasche A, Baronti C, Aldabbagh S, Cadar D, Reusken C. Clinical comparison,
standardization and optimization of Zika virus molecular detection. Bull World
Healt Organ [Internet]. Forthcoming. Available from: http://www.who.
int/bulletin/online_first/16-175950.pdf.
53. Kutsuna
S, Kato Y, Takasaki T, Moi M, Kotaki A, Uemura H, et al. Two cases of Zika
fever imported from French Polynesia to Japan, December 2013 to January 2014.
Euro Surveill. 2014;19(4) pii: 20683.
54. Hirayama
T, Mizuno Y, Takeshita N, Kotaki A, Tajima S, Omatsu T, et al. Detection of
dengue virus genome in urine by real-time reverse transcriptase PCR: a
laboratory diagnostic method useful after disappearance of the genome in serum.
Journal of clinical microbiology. 2012; 50(6):2047–52.
55. Barzon
L, Pacenti M, Franchin E, Pagni S, Martello T, Cattai M, et al. Excretion of West Nile
virus in urine during acute infection. The Journal of infectious diseases.
2013; 208(7):1086–92.
56. Pan American Health Organization. 2015. Epidemiological update. Zika virus infection. 16 October
2015. Pan American Health Organization, Washington, DC. http://www.paho.org/hq/index.php?option_com_docman&task_doc_view&Itemid_270&gid_32021&lang_en.
57. Allain JP, Bianco C, Blajchman MA, Brecher ME, Busch
M, Leiby D, Lin L, Stramer S. 2005. Protecting the blood supply
from emerging pathogens: the role of pathogen inactivation. Transfus Med Rev, 19:110–126.
58. Chen
LH, Hamer DH. Zika Virus: Rapid Spread in the Western Hemisphere. Ann Intern
Med. 2016; 164(9):613-5.